The 2026 IME Market Report
Executive Summary
We surveyed�claims professionals across the United States�to understand how Independent Medical Examinations (IMEs)���evaluations conducted by a neutral, third-party physician���are being used today, what drives their use, and what this reveals about the gap between where the market�currently is�and where it�needs to be.��
Three key findings define the current landscape:�
The market is�stable but�carrying more weight per claim.��
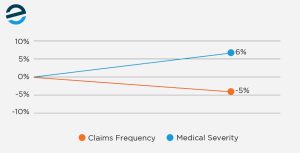
70% of respondents report no change in IME volume, yet medical severity�rose�by�6% in 2024�alone�and�remains�elevated�according to�the latest NCCI updates.�Fewer claims are reaching the IME stage,�and�the ones that do carry higher financial exposure.��
IMEs�are being used to resolve medical uncertainty, and expectations need to reflect that.�
When asked what drives the decision to order an IME, 42% of respondents cited clarifying causation and resolving conflicting opinions.�When asked�to�identify�the single most valuable�outcome,�44%�pointed to a clear determination of causation.�When the goal is a defensible medical decision, quality becomes the priority, and higher-quality IMEs�require�more time and higher cost. That reality makes timing and expectation�setting�important early in the claim.�
There�s�a quality gap.��
More than�1 in�3�respondents rated their IME vendor a 3 out of 5 or lower.�Less than�1 in�5�gave�a�top�score. Slow turnaround, scheduling delays, and reports that lack clarity are the�most common�frustrations.�These issues point to a broader concern around consistency and report quality: vendors�optimizing�volume over rigor.��
These�key�findings suggest�that IME usage may be stable, but its role has become more concentrated. Claims that progress to an IME today�are�more complex and carry greater financial and legal impact, which raises the importance of reaching a clear and defensible conclusion. The survey data�indicates�the vendor market has not fully adapted to that reality, with performance patterns that continue to favor volume over the level of�analysis these claims demand.��

Section 1: A Stable Market Carrying Higher Stakes �
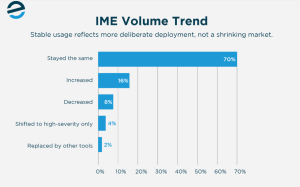
IME usage has held steady, with�70% of respondents reporting�no change in volume over the past 12 months.�That stability takes on a different meaning when viewed against broader claim trends.��
Claim frequency�declined�5% in accident year 2024, the third consecutive year of above-average declines,�while medical severity�increased by 6%, with recent updates�indicating�that�pressure on claims costs is continuing. For�high-cost claims exceeding $5 million,�medical expenses account for approximately 90% of total costs.��
Early-intervention protocols and medical-cost-containment regulations have also reduced escalation in simpler cases.�This includes faster claim reporting, earlier�contact with injured workers,�increased�use of nurse case management, and tighter controls around treatment authorization and provider�selection. These steps resolve many routine issues before they develop into larger disputes.�As a result, more straightforward claims are resolved earlier and do not progress to the IME stage.��
With fewer claims overall, stable IME volume�suggests�that examinations are being used�consistently, but�within a�narrower�portion�of the claim population. A larger share of IMEs is now tied to higher-severity claims with greater�financial impact.�This points to a shift toward more selective use, even if overall volume�remains�unchanged.��

Section 2: Why IMEs Get Ordered � And What That Tells Us�
When claims professionals order an IME, they are�trying to resolve�a medical narrative that is unclear, incomplete, or contested.�That has not changed.��
Causation and conflicting opinions account for 42% of all cited ordering reasons. This�remains�the primary driver, ahead of�litigation defense, cost control, and severity combined. That�priority�carries through to outcomes � 44% of respondents say clear causation determination provides the most value from an IME.

Medical opinions�frequently�diverge, and that divergence is often centered on causation and work-relatedness, which is exactly why IMEs exist.��
The role of�an�IME�has�remained�consistent:�to answer a medical question that directly affects how the claim moves forward.�What has changed is where�the question�is addressed. In many cases, it is no longer the first step.��
Lower-complexity claims are increasingly resolved earlier through tools like peer review,�utilization�review, and nurse case management.�By the time an IME is introduced, the file has often already been evaluated, and the remaining issue is more disputed or more consequential.��
This creates a�higher expectation�for what a quality IME must deliver.�A causation determination�on a routine claim carries limited impact, while that same determination on a high-exposure claim can influence reserve decisions and litigation strategy.�
Section 3: What Is�Shifting�IME Behavior��
The market narrative�often�cites�technology as the primary�driver of change in the IME market�� AI,�analytics, telemedicine, and digital transformation.�While these forces are at play,�adjusters�report that day-to-day shifts are more closely tied to workflow decisions.��
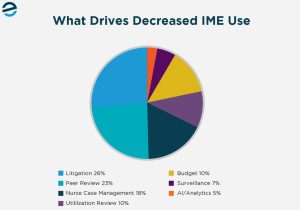
Among respondents who reported decreased IME usage, litigation strategy shifts (26%) and increased peer review (23%) were the top picks. AI and analytics tools accounted for just 5% of responses. The changes happening in practice are driven by how a claim is being litigated and whether a paper-based review�or�nurse�case management�is sufficient before escalating to a full examination.��
In many cases, peer review is used to�determine�whether�a formal exam is necessary, helping control�costs�and avoid over-deploying�IMEs on straightforward claims. At the same time,�litigation�strategy is shaping when IMEs are ordered, with exams more often reserved for cases where the opinion will directly�impact�defense, settlement,�or�trial outcomes.��
So,�the question becomes: when is a peer review enough, and when does a claim require an IME?��

Peer Review vs. IME: Knowing When Each Tool Belongs��
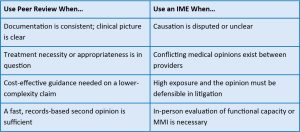
Peer review and IMEs serve�different�functions,�and�conflating them creates risk. Peer review is a records-based assessment, often used when the medical record is complete and internally consistent.�It�provides a faster opinion at a lower cost in lower-complexity claims, where a full examination may not add meaningful value.��
An IME�requires a physical evaluation by an independent physician and produces an opinion grounded in direct clinical observation.�It becomes necessary when the file does not resolve the core issue, especially in cases involving disputed causation or conflicting medical opinions.�Because it involves scheduling, exam time, and a detailed report, it takes longer and costs more than peer review, but that added time and�expense�are what allow the physician to assess credibility and apply clinical judgment in a way the record alone cannot.��
Survey findings suggest increased reliance on peer review as�an initial�clinical filter.�This�aligns�with broader�workers� compensation trends toward�utilization�review, nurse case management,�and file-based physician assessment before pursuing�the�more costly, time-intensive IMEs.�However, peer review is unlikely to�replace IMEs�in complex or disputed cases;�rather,�it is�more often�used�to�determine�whether an IME is�truly necessary.��

Section 4: The Quality Gap � Where the Market Falls Short**�**�
Satisfaction with IME vendors is far from strong ��1�in�3�respondents rated their�vendor�average or�worse, while fewer than 20% gave a top score. That gap suggests IME providers are clearing the bar on�basics, but�falling short when it comes to the clarity and efficiency that claims really demand.

The top complaints are operational: slow report turnaround (18%), scheduling delays (16%), and reports that lack clarity (14%). Opinions not defensible in litigation (10%) and difficulty finding the right specialist (9%) follow closely behind.��
Scheduling constraints are, in part, a structural problem. The AAMC projects a shortage of up to 86,000 physicians by 2036, with surgical specialties among the most affected. These specialties are among the most in-demand for�IMEs and the most difficult to schedule. Physician availability directly limits what any vendor can deliver in terms of timeline.��
But the complaints about clarity and defensibility signal something far more fundamental.�

The Deeper Problem: Volume Over Rigor��
IME vendors�operating�at scale often�prioritize speed and geographic coverage. This means�larger physician panels, standardized workflows, and faster report turnaround targets, which�improve efficiency�but can limit the depth of analysis in more complex cases.��
The result is reports that are completed quickly but rely on generalized language or incomplete clinical integration. When a report does not fully address the referral question,�it creates another decision point. That can�mean�follow-up reviews, supplemental questions, or a second IME�before anything can move forward.��
Research supports what adjusters are experiencing firsthand � IME quality is not consistently applied across examinations, with documented gaps in patient-centered analysis and integration of clinical information. The AMA Guides and ACOEM set a clear standard: medical opinions grounded in evidence-based medicine and reasoned, case-specific analysis. But�in high-volume environments,�maintaining�that level of rigor becomes more difficult.�
This creates a tradeoff across the market. Vendors focused on speed and cost tend to deliver faster turnaround times. Vendors focused on quality tend to require more time and higher cost. The difference�shows up in�whether the IME resolves the issue or extends the claim.��
Section 5: What A Good IME Vendor Looks Like�
The characteristics that distinguish vendors who consistently clear that bar are not complicated, but they require intentional investment that volume-first business models may not prioritize.��
Physician Vetting: More Than a License Check�
Good physician vetting means confirming the physician is actively practicing, holds the right specialty for the claim at hand, and has no history of sanctions or exclusions.�It�s�also important to consider the physician�s practice mix. Courts may scrutinize opinions from physicians who perform a high volume of insurance work, so vendors with rigorous, balanced vetting protocols help ensure that reports are well supported and more likely to withstand challenge.��
Report Quality Assurance: The Question That Has to Get Answered��
A quality assurance process should check whether the physician addressed the specific referral questions, whether the reasoning is grounded in the clinical findings, and whether the conclusions would survive cross-examination. A report that restates the medical record without drawing a defensible conclusion�hasn�t�done the job, regardless of how quickly it arrived.��
Specialty Depth, Not Just Panel Size�
A large physician network is only useful if the right specialist is available for your specific claim. When causation is disputed or the injury is complex, a vendor�s ability to match you with the right examiner, not just the nearest one, makes a major difference in opinion quality.�
Proactive Communication as a Standard�
Much of the friction behind the top complaints in our survey stems from simply not knowing where a claim stands. A vendor that keeps you informed at each step saves your team�significant time�and reduces the back-and-forth that compounds�delays.�

Section 6: What Claims Professionals Should Do Now�
1. Match the tool to the question�
IMEs are most effective when the claim outcome depends on resolving a clinical question with high exposure attached. In cases where documentation is consistent and the clinical picture is�clear,�peer review or�utilization�review may be the right first step. But deploying the wrong tool for the situation only creates�more problems�downstream.��
Using an IME in a low-complexity situation adds time and cost without improving the outcome. Using peer review in a complex situation can delay resolution and create�additional�steps later.�The goal is to avoid introducing a second decision point.��
**2. Be deliberate about timing **�
Timing directly�impacts�whether an IME provides value. If the clinical picture is still evolving, the report may not�provide�a clear answer. If the IME is ordered too�late, the claim carries unresolved exposure longer than necessary.�The trigger for ordering should be a considered decision based on where the claim stands, not a default response to stagnation or an arbitrary stage in the claim lifecycle.�
Ordering earlier in the decision-making�process increases�the likelihood of a usable outcome, especially when�it is clear that causation�or conflicting opinions will not�resolve�on their own.��
Timelines should also reflect the type of examiner�required. Specialists are more difficult to schedule and often require longer lead times. Higher-quality IMEs, particularly those involving the right specialist, take longer and cost more. Setting realistic�expectations�early helps avoid delays later in the claim.��
3. Evaluate your vendor relationships with the same rigor you�d apply to the claim�
The survey data�suggests many claims�professionals�are working with results that do not fully meet expectations.�Vendor performance should be measured by whether the IME resolves the question the first time.��
Faster, lower-cost exams may appear efficient, but if they lead to�additional�reviews or repeat IMEs, total claim�duration�and cost increase.�Actively evaluating vendor performance � and being willing to act on what you find � yields outcomes more likely to justify the investment.��
�
Sources�
American Medical Association. (2025, December 4).�AMA Guides� to the Evaluation of Permanent Impairment: an overview. AMA.�https://www.ama-assn.org/practice-management/ama-guides/ama-guides-evaluation-permanent-impairment-overview��
Association of American Medical Colleges. (2024, March).�The Complexities of Physician Supply and Demand: Projections From 2021 to 2036.�AAMC.�https://www.aamc.org/media/75231/download��
Currey, J., &�Sprogis, S. K. (2024, October 24).�Conceptualising�the quality experience for independent medical examinations: A narrative review. ScienceDirect.�https://www.med.upenn.edu/pmi/events/https-www-sciencedirect-com-science-article-abs-pii-s1047847720300046-via-3dihub��
National Council on Compensation Insurance. (2024).�2024 Regulatory and Legislative Trends Report. NCCI.�https://www.ncci.com/Articles/Documents/II_Regulatory-Legislative-Trends2024.pdf��
National Council on Compensation Insurance. (2025, May 13).�2025 State of the Line Guide. NCCI.�https://www.ncci.com/SecureDocuments/SOLGuide_2025.html��
Pitfalls during times that compromise IME reports. Weber Legal Nurse Consulting Inc. (2024, December 31).�https://www.weberlegalnurse.com/pitfalls-during-times-that-compromise-ime-reports��
Rohom, K. (2026, April).�Independent Medical Evaluation Service Market Size 2026-2032. 360iResearch.�https://www.360iresearch.com/library/intelligence/independent-medical-evaluation-service